Clinical Cases to Challenge, Teach, and Refine Your Ophthalmic Practice
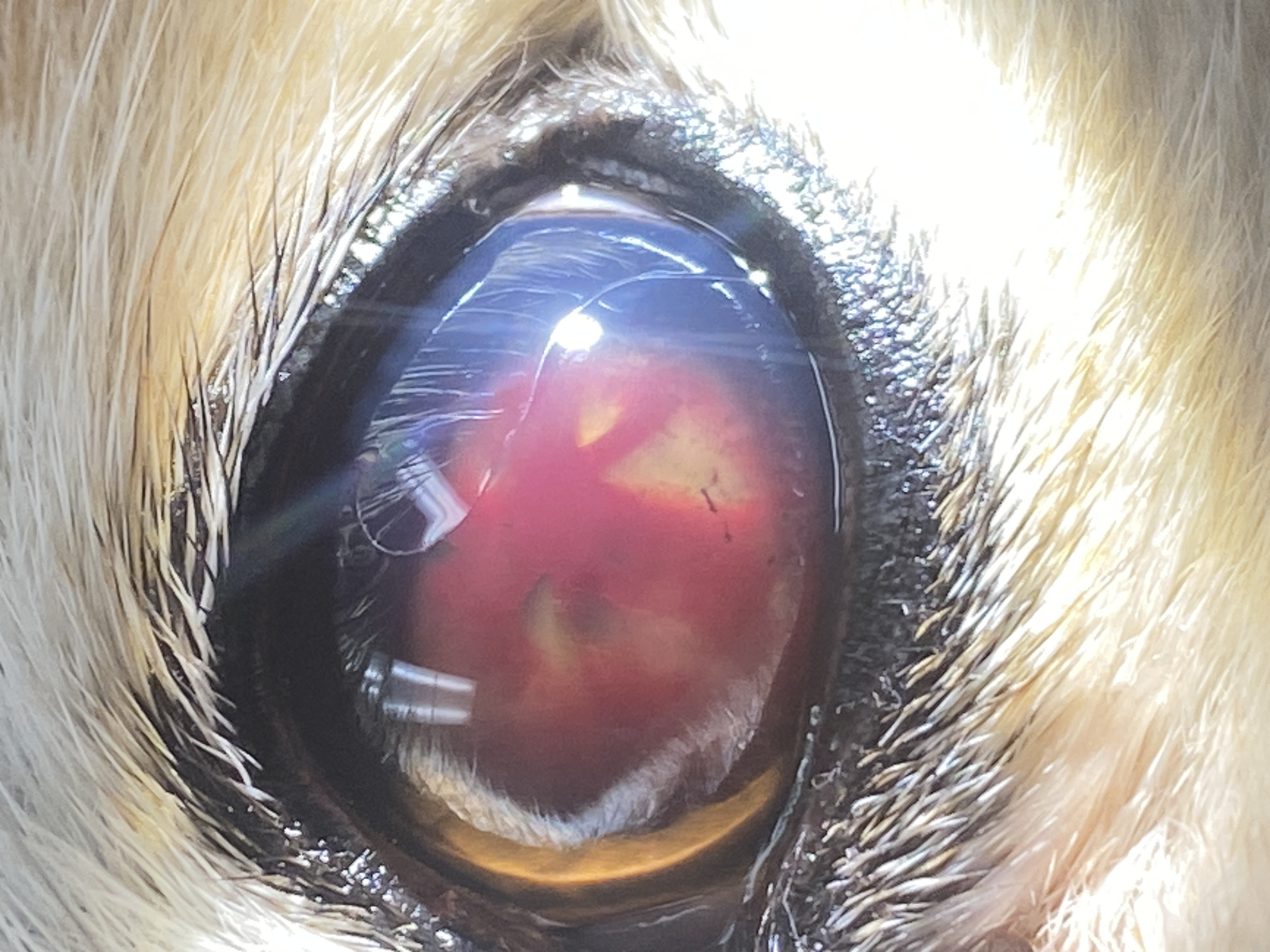
Welcome to a curated collection of real-world ophthalmic cases drawn from clinical practice. Each image is paired with a focused clinical insight and a key takeaway designed to sharpen your diagnostic thinking and refine your treatment approach. From corneal ulcers and hypopyon to uveal cysts, hyphema, and beyond, these cases reflect the complexity and nuance that defines veterinary ophthalmology in practice.
Whether you're a seasoned clinician or still building your ophthalmic confidence, this page is designed to challenge assumptions, highlight the findings that matter most, and prompt the kind of critical thinking that changes outcomes. Each case invites you to look closer, consider the differential, and ask what you might have missed.
Scroll through, engage with the questions, and test your clinical instincts — because in ophthalmology, what you see is only the beginning.